Take time out of your busy day and make a Donation to an amazing cause. Shed some light on Heart Awareness

Heart failure affects approximately 500,000 Australians, with around 67,000 new diagnoses each year.¹
Despite its prevalence, many Australians remain unaware of the signs and symptoms, or the important role that other health conditions can play in heart failure risk and progression.
Heart failure rarely exists in isolation. Many people living with heart failure are also managing other health conditions such as kidney disease, type 2 diabetes, high blood pressure, obesity and mental health conditions.² Understanding these connections can help people seek support earlier, improve management, and achieve better health outcomes.
Heart failure does not mean the heart has stopped working. Heart failure occurs when the heart is unable to pump blood effectively enough to meet the body’s needs.³
It is a serious and progressive condition that can affect a person’s quality of life and lead to frequent hospitalisations if left unmanaged.
Heart failure affects around half a million Australians and results in approximately 158,000 hospital admissions every year.
Many people are surprised to learn that heart failure is closely linked to other chronic health conditions. These are often referred to as connected conditions because they frequently occur together and can influence one another.²
Common connected conditions include:
Chronic kidney disease
Type 2 diabetes
High blood pressure
Obesity
Mental health conditions
When one condition worsens, others can often follow, making management more complex and increasing the risk of poor health outcomes.²
Kidney disease is one of the most common, serious and under-recognised connected conditions associated with heart failure.² Nearly half of people living with heart failure are also living with chronic kidney disease.4
The heart and kidneys work closely together to keep the body functioning properly. When one organ is affected, it can place additional strain on the other.4
Because kidney disease can develop silently over time, many people may not realise they are living with it until it has progressed.
Living with heart failure can affect every aspect of daily life, particularly when other health conditions are involved. Watch Adam’s story to learn about his experience living with heart failure and kidney disease.
Heart failure symptoms can develop gradually or appear suddenly.5 They are often mistaken for other health conditions, which can delay diagnosis and treatment.
Common symptoms may include:5
Breathlessness
Fatigue or reduced energy levels
Swelling in the legs, ankles or abdomen
Sudden weight gain
Difficulty sleeping when lying flat
Persistent coughing or wheezing
Recognising symptoms early and speaking with a healthcare professional can help people access appropriate care sooner and improve long-term outcomes beyond health, which can include the financial burden of managing heart failure.²
Keeping track of symptoms can help you better understand changes in your health and support conversations with your healthcare team.
If you are experiencing symptoms of heart failure, or are living with kidney disease, diabetes or high blood pressure, speak with your GP or healthcare professional.
Early detection and proactive management can help improve outcomes and quality of life.
 Learn the signs and symptoms of heart failure
Learn the signs and symptoms of heart failure
Understand how connected conditions can affect heart health
Ask your healthcare professional about heart and kidney health checks
Download the Heart Failure Symptom Tracker
Share this information with family and friends
Heart Failure Awareness Week is a Hearts4heart initiative that aims to improve understanding of heart failure, promote early detection, and support Australians living with heart failure and connected conditions.

Footnotes:
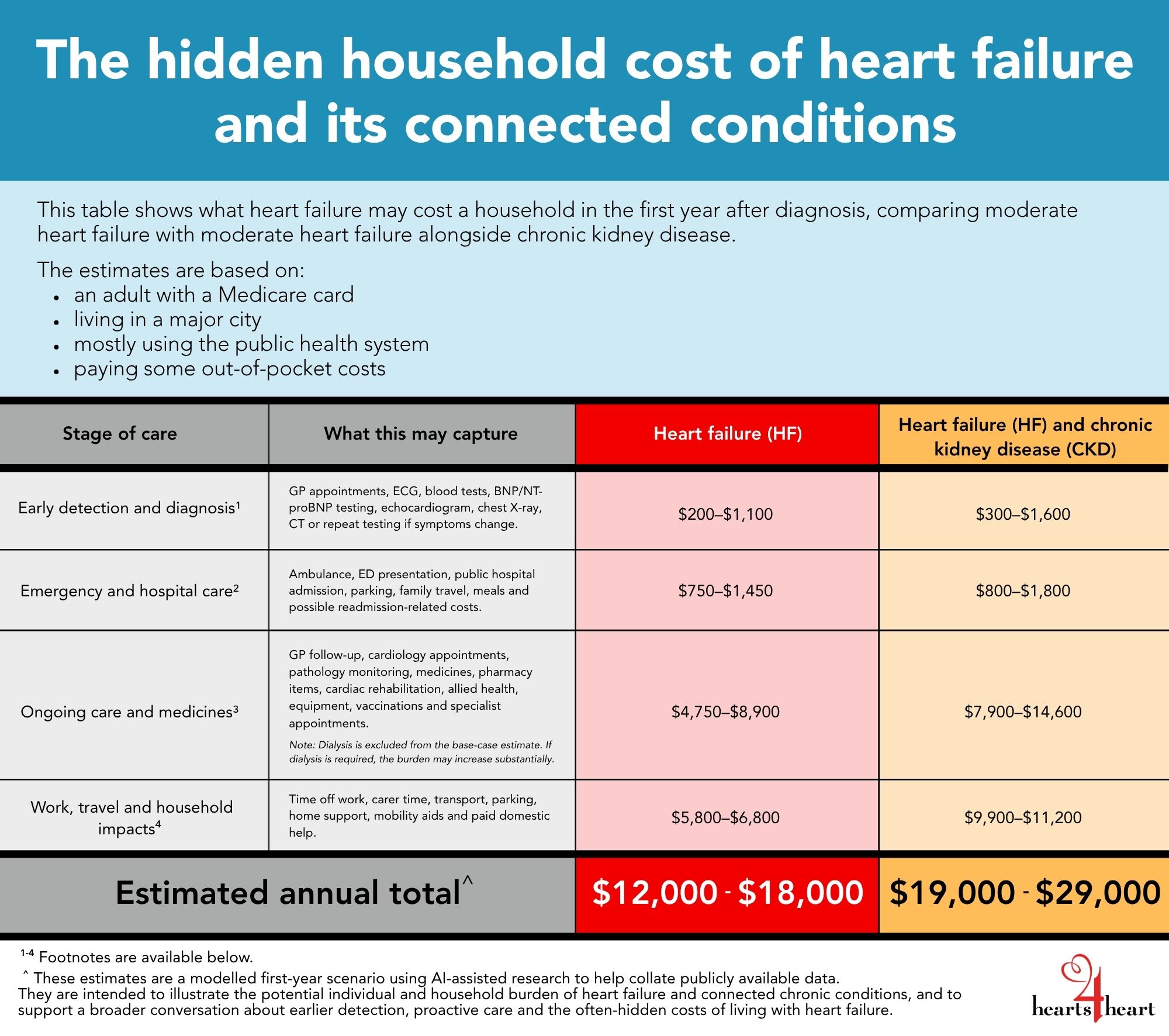
¹ Early detection and diagnosis
This section includes GP appointments for symptoms, heart check, referral and results; ECG; blood tests including kidney function and electrolytes; BNP/NT-proBNP testing if used; echocardiogram; chest X-ray; CT or other imaging where clinically appropriate; and repeat testing if symptoms change.
The estimate is built from the Phase II line-item model, including GP visits modelled at a $50 out-of-pocket gap per non-bulk-billed visit; ECG ($0-$30); blood tests ($0-$100 for HF and $0-$200 for HF + CKD); BNP/NT-proBNP ($0-$100); echocardiogram ($0-$150); chest X-ray ($0-$80); CT/other imaging where clinically appropriate ($0-$300); and repeat testing if symptoms change.
Relevant reference links include MBS item 66830 for BNP/NT-proBNP testing, MBS item 55126 for transthoracic echocardiography, and Kidney Health Australia/Deloitte CKD modelling for CKD monitoring assumptions.
² Emergency and hospital care
This section assumes one ambulance event and one public hospital pathway for a Medicare-eligible public patient. Public ED presentation and public hospital admission are modelled as $0 direct hospital bill, but this does not mean the event is cost-free to the household. Ambulance, transport, parking, family travel, meals and possible readmission-related costs are captured separately.
The ambulance estimate uses a rounded $600 proxy due to state variation. NSW Ambulance lists a call-out fee plus per-kilometre charge from 1 July 2025; actual costs may be $0 or higher depending on state, ambulance cover, concession status and distance.
Relevant reference links include the Australian Government overview on Medicare billing in public hospitals and NSW Ambulance accounts and fees. Private hospital ED fees, private hospital excesses and private inpatient costs are excluded from the base case.
³ Ongoing care and medicines
This section includes GP follow-up and medication review, cardiologist appointments, additional specialist appointments where relevant, repeat pathology monitoring, repeat cardiac imaging if clinically required, PBS medicines, non-PBS pharmacy costs, cardiac rehabilitation, allied health, at-home monitoring equipment and recommended adult vaccinations.
The GP visit assumption has been strengthened using SHAPE data. The SHAPE healthcare-use study found people with definite or probable heart failure attended GP practices 14.4 times per year on average, with frequency increasing with comorbidity burden. The model therefore uses 12-14 GP follow-up/medication review visits for HF and 18-20 visits for HF + CKD.
Medicine costs use the 2026 general PBS co-payment of $25 per script for Medicare card holders, with a higher medicine burden modelled for people living with both heart failure and CKD. Pharmacy costs also allow for non-PBS, over-the-counter and complementary medicines, delivery, dose aids and brand premiums. Vaccination costs are included as a conservative modelled line item because some vaccines may be recommended but not fully funded for every adult, depending on age and eligibility.
Relevant reference links include the SHAPE healthcare-use study in AJGP, the SHAPE epidemiology study, PBS co-payment information, Australian Government adult immunisation guidance, Medical Costs Finder, and Kidney Health Australia/Deloitte CKD modelling for CKD and nephrology assumptions.
⁴ Work, travel and household impacts
This section captures household costs that may not appear on a medical bill: time off work for appointments, tests and recovery; unpaid carer time; transport to appointments; parking; minor home modifications or mobility aids; and paid domestic support where required.
Work and carer time are modelled as a productivity/time burden, not always a direct cash payment. The calculation uses an Australian average full-time earnings proxy to estimate the value of missed work time or unpaid carer time. This means the figure will apply differently depending on whether the person is working, retired, casually employed, self-employed, supported by family, or relying on unpaid care.
Transport and parking are modelled using conservative metropolitan assumptions. Costs may be higher for people in regional or rural areas who need to travel further for cardiology, imaging, nephrology, rehabilitation or other specialist care.
Relevant reference links include Australian Bureau of Statistics Average Weekly Earnings for wage-based proxy calculations and Kidney Health Australia/Deloitte CKD modelling for CKD-related transport, non-prescription and household cost assumptions.
The model is based on:
• an adult Australian Medicare card holder
• living in a major city
• accessing care mainly through the public system
• some mixed-billing out-of-pocket costs
• moderate heart failure in the first 12 months after diagnosis or hospitalisation
• moderate-to-advanced CKD requiring additional monitoring and nephrology input in the HF + CKD scenario
• no dialysis in the base-case HF + CKD estimate
Actual costs may be lower for people who are bulk billed, have concession cards, have ambulance cover, receive care entirely through public outpatient clinics, or do not require all tests, appointments or supports included in the model.
Actual costs may be higher for people who use private specialists or private hospitals, pay private hospital ED fees or excesses, require more frequent testing or imaging, live in regional or rural areas, need paid care or home support, experience readmission, or live with multiple comorbidities.
References
